Red light therapy for osteoarthritis: just hype or real hope?

Interest in red light therapy for a variety of clinical conditions and health applications is surging. Your favourite health and longevity influencers have likely either posted some red light therapy related content or included a red light therapy brand as one of their advertisers.
There is even a whole podcast devoted to red light therapy (of course with industry affiliations).
According to data from Glimpse, as of March of 2025, google search interest grew by 59% compared to the previous year, reaching approximately 2.5 million searches per month. And back to 2022 there were on average less than 0.5 million searches per month. It’s fair to say the red light hype machine is in full motion.
And you know it’s a full on trend when mom and dad are using it, too! I was home this past weekend and they showed me a unit that had been passed on to them to try. Dad gave it glowing reviews for helping him manage his advanced knee osteoarthritis. 30 minutes a day, seemed to improve his knee pain and help him get on with his day.
It left me wondering, what is truth and what is hype when it comes to red light therapy and osteoarthritis and how is red light therapy similar or different than the class 4 laser we use in clinic?
In our experience managing various types of osteoarthritis cases, class 4 laser can be a good adjunct therapy to a comprehensive rehabilitation plan.
Is it possible patients can now get a similar treatment effect with at-home red light therapy units?
Disclaimer: this is not an exposee on red light therapy as a whole. There are simply too many clinical applications to review. The most exciting and promising results appear to be related to eye and skin disorders, not our area of specialty! For a comprehensive understanding of red light therapy for different clinical conditions check out Dr. Rhonda Patrick’s page.
For a foundational understanding of how light therapy (including sunlight and blue light) can affect our health check out Andrew Huberman’s podcast called “using light to optimize health” from 2022. It’s a fascinating listen…so good, I recently listened to it for a second time.
What is red light therapy?
Red light therapy uses specific wavelengths of red or near-infrared light to stimulate cells and tissues, triggering a range of biological responses.
The wavelengths of different colours of light are measured in nanometres. The spectrum of visible light is approximately 380nm to 750nm as shown below.
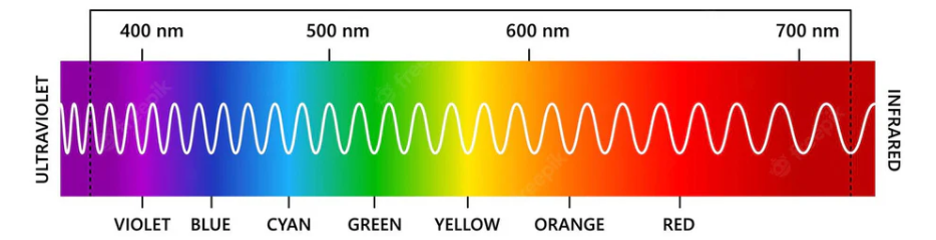
Red light (around 620-750 nm) and near-infrared light (750-1100 nm) are considered longer wavelength light which can penetrate the skin and it may be able to boost energy production at a cellular level on various tissue levels.
Most clinical studies using red light and near-infrared light therapy occur between 650nm and 1000nm, sometimes termed the “optical window” known to be capable of stimulating cellular activity.
Think of it as the human parallel of photosynthesis, where plants use energy from sunlight to create chemical energy…which you will of course remember from Grade 9 biology 🙂
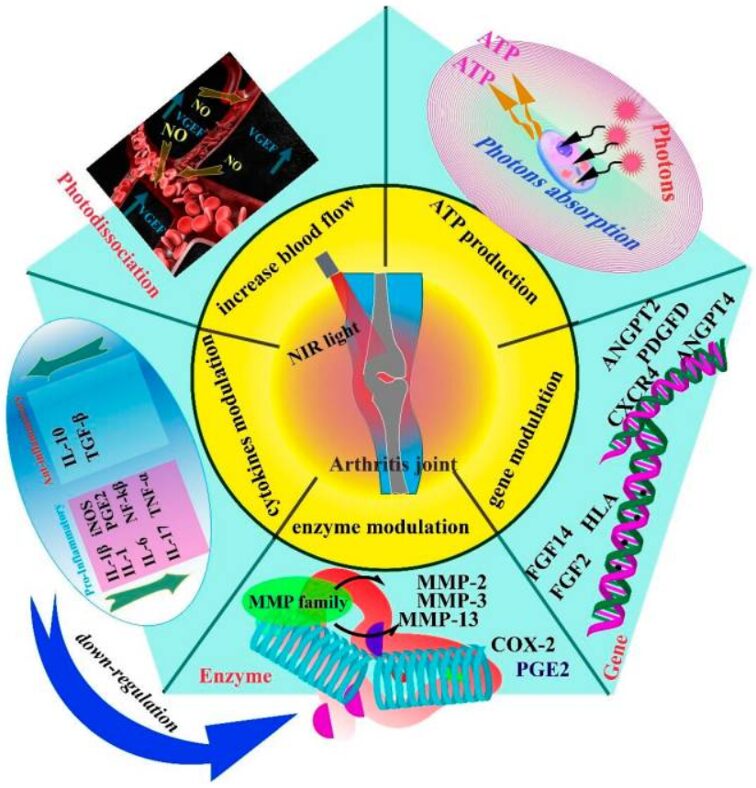
Photobiomodulation and osteoarthritis
A 2023 review proposed 5 key areas of photobiomodulation, the clinical use of red and near-infrared light, can exert a therapeutic effect for arthritis: increases blood flow, ATP production, gene modulation, enzyme modulation and cytokine modulation.
These benefits are primarily from animal (rat) based studies, which have been accelerated into osteoarthritis in various ways. Several rat trials also show some promise in cartilage recovery.
But we need human trials to have any confidence in a clinical recommendation. And although human trials on the therapeutic effects of photobiomodulation and osteoarthritis have yielded some encouraging results with reduction in pain, swelling and morning stiffness there have also been several studies that have reported no effect or minimal effect.
Thus treatment parameters (such as wavelength, treatment power and light source) need to be considered when evaluating clinical efficacy.
To understand the varying clinical outcomes in these trials we need to differentiate between the types of photobiomodulation: low level laser therapy, high intensity laser therapy and red light therapy.
Different types of photobiomodulation: Low level Laser, High-intensity laser and Red Light Therapy (LED)
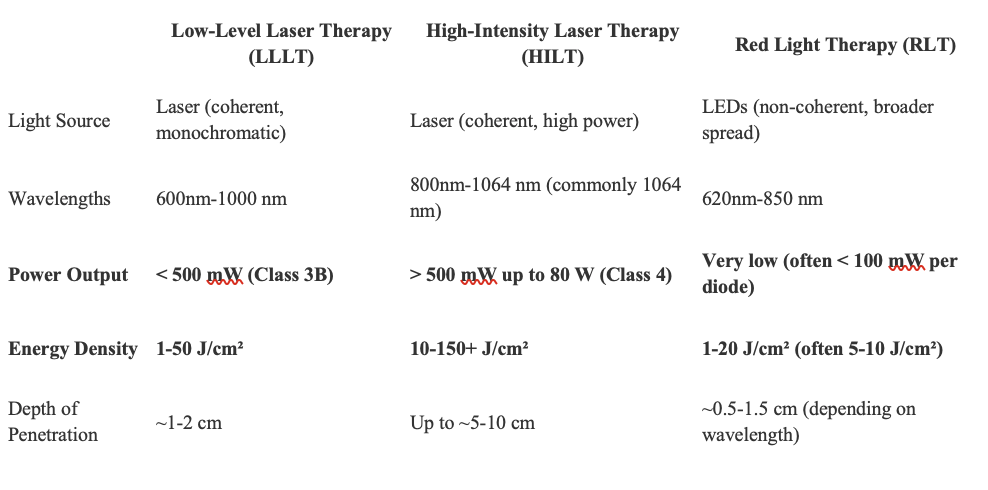
Red light therapy and laser therapy share some characteristics (using similar bandwidths of near infrared light in some cases), however there are several important differences.
Red light therapy originates from LED’s (light-emitting diode) which emit light when an electric current passes through a semiconductor. The design is simple and can be easily mass produced. LED uses multiple wavelengths of light, and are typically lower in power. A typical at home unit (ie. Juuv and Kala) costs around $500.
Lasers require more complex components like precisely aligned mirrors and gain mediums to emit photons of light in a synchronized, coherent manner. They also often require robust cooling systems and power supplies. Lasers are often manufactured in smaller quantities for more specialized applications and often require precise calibration and certification, adding to the cost. Lasers can be low powered (Class 3 lasers) or high powered (Class 4 lasers). In Canada Class 4 lasers power output is in the range of 0.5W to 80W compared to low level lasers (Class 3 lasers) that are under 0.5W. Red light therapy units are typically in the range of 100mW.
Class 4 lasers start at $30,000, with many newer 50+W units well over $50,000.
The importance of light coherence of lasers versus red light therapy has been suggested to be of much lower significance compared to the wavelength of the light and the power as summarized in table 2 of the animal (mice) arthritis models.
The power of the unit determines the amount of energy that can be delivered to a specific area of tissue, measured in joules per square cm (J/cm2).
Low-Level Laser Therapy for osteoarthritis
A recent review identified 15 human trials that test low level laser therapy with primarily knee and hand osteoarthritis.
As displayed in table 4, the clinical questions were highly varied from short term results, to long term results and prevention of knee replacements.
The majority (11 of 15) of the studies concluded low-level laser demonstrated favourable outcomes with low level laser therapy. There was considerable variability in how low level laser was applied which may results in the variations in outcomes.
High-intensity Laser Therapy for osteoarthritis
A recent systematic review and meta-analysis of high intensity laser therapy for knee osteoarthritis, which included 9 trials, concluded high intensity laser therapy could be a promising modality in alleviating knee osteoarthritis pain, especially when combined with exercise therapy.
Again there was considerable variability in trial methods including power output, total energy delivered and patient positioning/laser application sites.
High intensity laser versus low-level laser for osteoarthritis: does the dose matter?
In short, yes, the dose of energy delivered to the osteoarthritic joint does matter.
A recent review identified five trials comparing high intensity laser therapy (HILT) versus low level laser therapy, either as a stand alone treatment or with associated physical exercise for knee osteoarthritis.
Compared to placebo, both LLLT and HILT demonstrated significant improvement in pain scores and functional improvement, with significantly better results for HILT.
One high quality, double blinded randomized controlled trial found negligible improvements for low level laser therapy when added to a 12 week exercise program. Comparatively high intensity laser therapy demonstrated a significantly measurable improvement in pain, function (timed get up and go test and KOOS scores) and range of motion when added to a 12 week exercise program.
The clinical effect of higher intensity laser therapy for pain and functional improvement for knee osteoarthritis is superior to low level laser therapy.
A low level laser therapy (Class 3 lasers) may have a small a small clinical effect, but is it clinically meaningful for most patients?
What about red light therapy for Osteoarthrits: where are the human trials?
A single trial of 50 elderly people with degenerative osteoarthritis demonstrated receiving red light therapy (red and infra red vs placebo) experienced pain reductions of over 50% after 10 days of treatment. This was a decent initial trial with some promising results, but had high potential for bias.
That trial was published in 1992 and is commonly referenced by red light therapy manufacturers. But 33 years have passed, where are the follow up trials??
This was somewhat surprising and so I consulted back with the aforementioned review page by Dr. Rhonda Patrick, which references several trials that demonstrate the benefits for photobiomodulation for osteoarthritis. But when you dig into each of those trials, they are all using a form of laser therapy and NOT red light therapy.
Red light therapy is seemingly flying on the coattails of the success from laser trials when it comes to osteoarthritis treatment.
We simply need more research to determine if red light therapy can deliver on its promises with respect to osteoarthritis.
What does AI say about red light therapy for osteoarthritis?
As a fun aside, ask your favourite AI platform whether red light therapy is effective for osteoarthritis. It will be an overwhelmingly positive response listing all the potential benefits and will make you want to buy into red light therapy.
But when you probe it to differentiate between the types: red light, low and high intensity laser and ask whether the power and dose of energy determines the clinical efficacy, then you start to see the nuance in the answer.
Make sure you follow their references with a skeptical eye, the confusion between laser therapy and red light therapy runs deep.
It’s a good example of needing to know how and what to prompt to get an accurate answer.
Dave’s take home on red light therapy for osteoarthritis
We simply don’t know at this point whether red light therapy can play any role in the management of osteoarthritis. There is biological plausibility (potential for benefit) and minimal risk, so go ahead and try it.
I suspect there is some small benefit similar to low-level laser therapy when it comes to easily accessible joints, ie hands, knee and ankle. So if you can harness that small benefit daily, that may be a great option for you to keep active.
For osteoarthritis of the low back or the hip or the shoulder, there is too much soft tissue for the light energy to penetrate and it won’t reach the joint with an adequate dose. The same issue applies to Class 4 lasers and we rarely try and target these deep joint issues.
Ultimately the burden of proof lies with these manufacturers of red light therapy products to prove the results they claim and stop riding the coattails of laser research results. Until that happens, don’t believe the marketing hype when it comes to red light therapy for osteoarthritis.