Does having low muscle mass cause osteoarthritis of the knee?

We are on an osteoarthritis article kick here at TPA. Does that mean Pete and I are getting older and we are selfishly spending time on issues pertinent to our own health?!?
While that may be a factor, I would submit to you that a bigger factor is the quality of research that is getting published in this topic area; likely owing to our aging baby boomer population and funding for research impacting this demographic.
Don’t blame us, blame the boomers 🙂
Pete summarized an article recently that demonstrated a whopping 43% reduction in your chances of developing symptomatic osteoarthritis of the knee if you were a “lifetime cyclist”.
He argues that the role cycling plays in helping manage your weight may be a key factor.
Some of you may be saying sure, we all know cycling is good for your knees, surgeon’s have been recommending non weight bearing exercise such as swimming and cycling for decades. “It’s the weight bearing exercise (walking, running, recreational sports etc) that causes the wearing and tearing.”
Well, now we have great data from the longitudinal Rotterdam Study, that adds some valuable nuance to this discussion.
The Rotterdam Study is a large population-based prospective cohort study that started in the 1990’s with the aim to describe the prevalence and incidence of multifactorial diseases in mid-life and the elderly. As of 2020 there were almost 18,000 Danish participants aged 40 and older who are examined and followed up with regularly. There have been hundreds of articles published from this dataset across a broad range of topics. It’s an impressive collection of epidemiological data across a broad range of health issues.
This particular osteoarthritis study was embedded within the Rotterdam study and included a cohort of 5003 participants followed on average just over 6 years to determine whether weight-bearing recreational physical activities are associated with increased risk of incident (new onset) knee osteoarthritis.
Patients within this study were 45 years or older, had baseline and follow-up knee x-rays and had regularly filled out validated exercise questionnaires and we followed for an average of 6 years. A subgroup of 1881 individuals also had their lean muscle mass measured by DXA (dual energy) scan at baseline. Of this group the authors lumped the participants into 3 lean muscle-index groups (low muscle mass, middle muscle mass and high muscle mass).
An example of which activities were classified as weight bearing or non-weight bearing activities is listed in table 1.
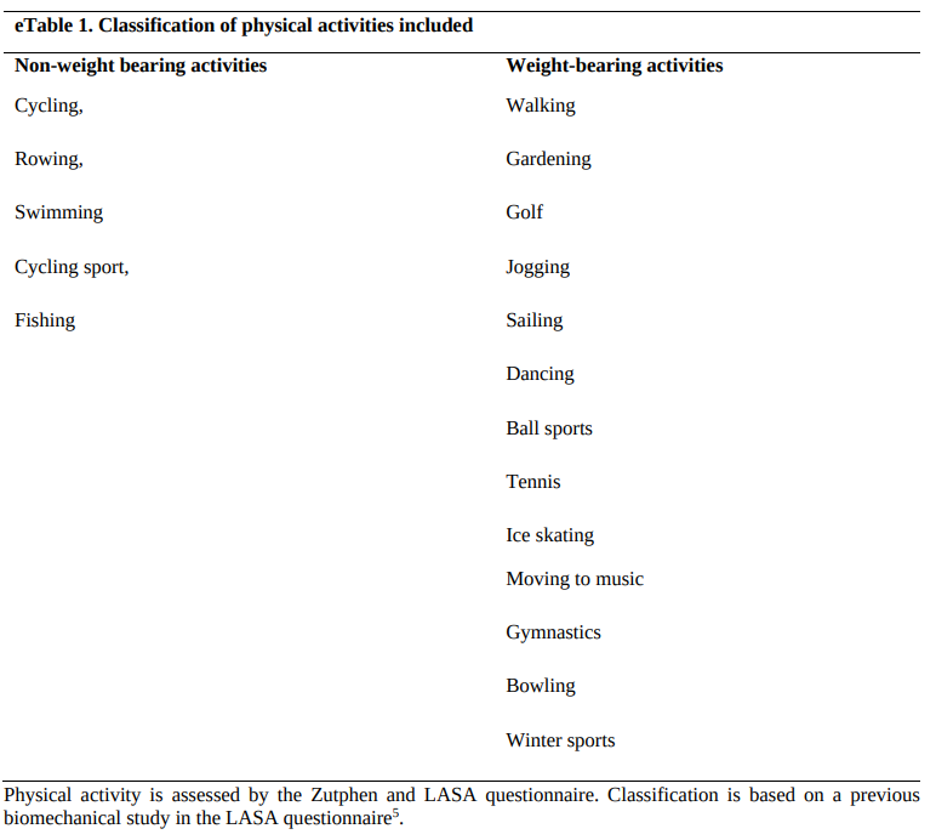
One of the main findings was an association between higher weight-bearing recreational physical activity and increased odds of incident radiographic knee osteoarthritis. This confirms the common medical advice that’s been recommended for decades, but also muddies the waters of the running doesn’t cause arthritis discussion.
Perhaps the nuance here is that not everyone is equally at risk of getting knee osteoarthritis from weight bearing activities. The authors found that in the subset of patients who had their lean muscle mass measured only the subjects in the low muscle mass group (not those in the middle or high muscle mass groups) had an observed increased associated risk of knee osteoarthritis from weight bearing activities.
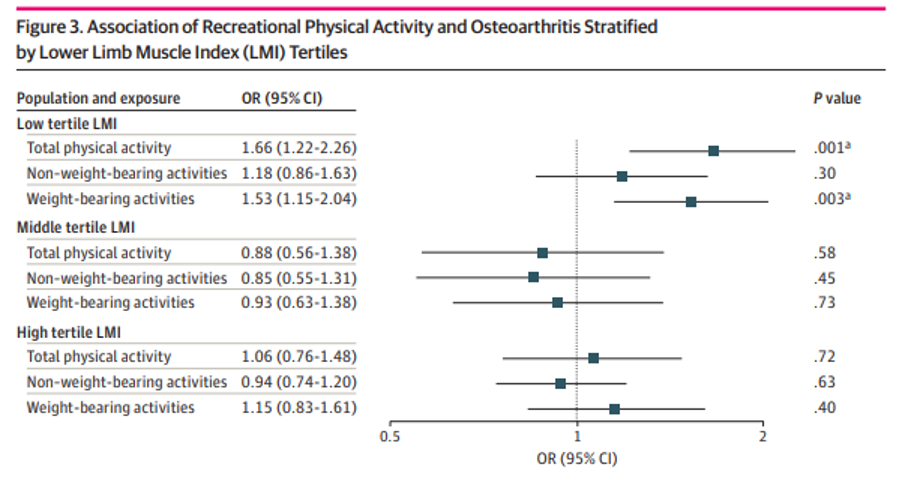
The proposed explanation is that with less muscle mass surrounding the knee joint there would be less load absorption from muscular system which may increase mechanical loading to the knee joint/cartilage.
This theory aligns with previous research has found that excessive mechanical loading can lead to increased matrix metalloproteinases and trigger several catabolic pathways leading to early osteoarthritis.
And also aligns with research that demonstrated knee muscle activation and thigh muscle strength decreases knee osteoarthritis risk.
Let’s be clear that this Rotterdam study is observational, and by it’s study design cannot answer the question of whether having higher muscle mass PREVENTS weight bearing activity from CAUSING osteoarthritis. This would be a costly, multiyear, large subject pool, controlled trial that realistically we are unlikely to see in our working years.
However this observed association is still very compelling, one that, in this authors opinion at least, puts lean muscle mass up there with obesity as a major modifiable risk factor worthy of significant clinical consideration.
How to figure out your knee osteoarthritis risk from this data?
2 things required to estimate this:
- Understand how low muscle mass was determined in this study
- Get your lean muscle mass measured via a DEXA scan (you can get this done locally, for about $100…reach out, we can help)
First off, the mean age of participants who were included in the subgroup analysis was 59 years of age. So if you are close to 59 years of age these lean muscle mass groups might apply and you can read below on how the lower limb lean mass index was calculated in the Rotterdam study. However for those of you significantly older or younger than 59 you may find more value in comparing your lean muscle mass to your age and gender matched peers. Check out this normative data chart below.
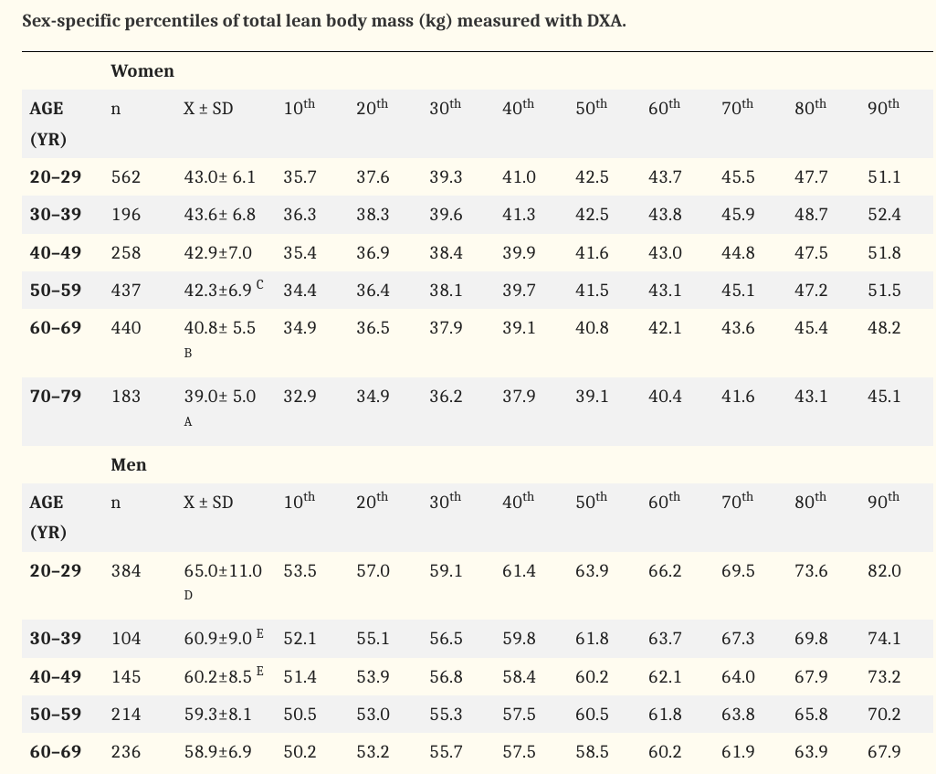
For clarity, I just want to highlight that this chart utilizes total body lean mass (in kg’s) measured with DEXA and the Rotterdam study used lower limb lean mass (in kg’s) only. When you get a DEXA scan it will provide both limb specific lean mass and total lean mass.
If anyone finds reliable age and gender matched normative data for lower limb lean mass please send it our way!
How lean muscle mass was calculated in the Rotterdam study
A lower lean mass index was used to define the 3 groups (high, middle and low muscle mass), which was calculated by lower limb lean muscle mass in kg found on the DEXA scan divided by an individual’s height, squared (kg/m2).
The lower limb muscle index of each group (low, middle and high) was not published in the study or provided with the supplemental data, however, a mean lower limb muscle index (LMI) of 5.57 across all subjects was described in the baseline data. So if we take a broader assumption that an LMI below 5.57 is low and above 5.57 is high it could look like the following:
If you are 5’2: below 13.78kg of lower limb muscle mass is low
If you are 5’8: below 16.57kg of lower limb muscle mass is low
If you are 6’2: below 19.64kg of lower limb muscle mass is low
Is Pete at risk of developing knee osteoarthritis from weight bearing activity?
Pete recently had a DEXA scan and was brave enough to allow me to use his numbers to highlight this topic.
Pete’s total lean muscle mass was 159.6 lbs. And his total lower limb muscle mass was 58.5lbs.
At just under 6’2” Pete’s lower limb muscle mass converted to kg’s would be considered high using the Rotterdam study LMI.
However, considering Pete’s age (much younger than you would assume from his grey head of hair) and the mean Rotterdam age (59), comparing his lower limb mean muscle mass to the Rotterdam data wouldn’t be appropriate.
Using the normative data chart above for total body lean muscle mass Pete would fall just shy of the 90th percentile for his gender and age matched (40-49) cohort. Nice work Pete….unlikely to need a knee replacement from all that running anytime soon. Disclaimer, this study did not account for the impact of head mass and Pete’s outrageously oversized head could be an additional problem 🙂
In conclusion, when it comes to the role of physical activity and developing osteoarthritis of the knee (and likely lower limbs at large) maybe instead of focusing on weight loss we should be focusing on lean muscle mass?