The single most important determinant of injury and rehabilitation from injury
Like the catchy title? Regretfully this is not a blog about some new enthralling gadget that can accurately determine who will get injured…..because nothing like this exists. There is one factor however that simultaneously both determines tissue injury and is the most important factor in injury rehabilitation – tissue load!
How important is the concept of tissue loading? Important enough that the International Olympic Committee put out an expert consensus statement this year to coincide with the Rio Olympics to update the world on the concepts of loading. (In fact they put out 2 consensus statements on it due to the sheer volume of information).
Load is way too large a topic to cover in a single blog post, so instead this blog will be on a new(ish) conceptual framework relating to load that has some fairly great data across a number of sports. This concept helps us determine who is at risk of injury, helps us predict potential injury, helps us appropriately return someone to their sport, and also will help coaches design appropriate training regimens for their athletes with minimal injury risk (I’m looking at you run and triathlon coaches!) Remember, training load related injuries are both common AND preventable.
Before introducing the acute:chronic work load ratio we have to understand a few concepts:
There are 2 types of load that each person experiences:
EXTERNAL LOAD: physical work. Examples are pitch count in baseball, run volume in any sport, jumps in volleyball etc. This one is easy to measure.
INTERNAL LOAD: a persons physiological or perceptual response. This one is much more difficult to quantify because it has to take into account individual factors. An example: There is currently some crazy person trying to run across the United States in under a month by completing a marathon daily. Comparing his physiological response to running 25km on a training day is far different then someone who is just embarking on a run training program and attempts to run 25km. Ideally, internal load is measured using a rating of perceived exertion or RPE (a scale of 1-10 for perceived training intensity). This intensity is then multiplied by the session duration to provide the persons ‘training load’. The unit is measured as RPE units x minutes. The unit is completely arbitrary however. It is an inexact measure of your body’s response to load. It is just meant as a measure of total training load. As an example in football, 300-500 units is considered a lower intensity training session while 700-1000 units is considered a higher intensity session. Of note, age is a huge determinant of internal load. It is outside the scope of this blog but keep in mind load perception based on individual age.
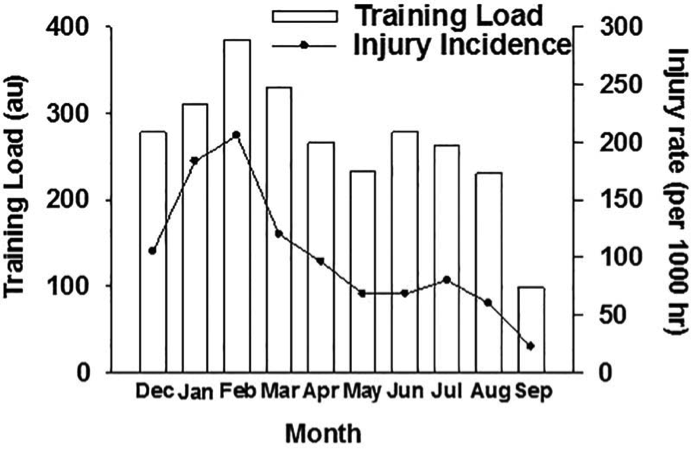
Now an ideal training load is one that will maximize an athletes performance while simultaneously limiting negative consequences of training like injuries, illness, fatigue, or overtraining. The issue is that while increased training loads will definitely improve a person’s performance, there is a dose related incidence of injury to higher amounts of loading. The chart below depicts this dose response relationship between training load and injury rate (this can be applied to essentially any sport). So how do we approach this problem?

The acute:chronic workload ratio is a convenient approach to this dilemma. The numerator, or acute workload (top number of the equation), is the persons total workload over the past 1 week. The denominator or chronic workload (bottom number) is a rolling average of the past 4 weeks of training. Using this equation gives the person a ‘preparedness factor’.
An easy example is a distance runner. If in the past 4 weeks they have averaged 40km of running at 5 minute km’s and, for our example, used a rating of perceived exertion of 3/10 for the entire time running. The denominator or chronic workload is 600 arbitrary units (5 minutes x 40km x 3RPE). Now, let’s say this person doubled their workload for the past week and upped their run volume to 80km at 5 minute pace with the same RPE of 3/10. Their acute workload is now 1200 arbitrary units. Therefore their acute:chronic workload is 2.0. If the same athlete had a chronic workload of 600 arbitrary units as stated above, however now is tapering for a race and runs just 20km at 5 minute pace at a RPE of 3, their acute workload is now 300 arbitrary units. This means the acute:chronic workload ratio is now 0.5.
That’s great but so what?
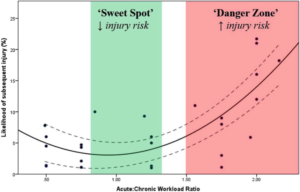
The acute:chronic workload ratio has now been used prospectively in a number of sports (a notably absent sport is running however – a sport which would likely have the longest reach across all athletes). It is suggested (in rugby, cricket, and Australian Rules Football) that if the ratio is kept under 1, the likelihood of injury in the next 7 days is as low as 5%. When the ratio is 1.5 or greater, the risk of injury is 2-4 times greater in the next 7 days. Therefore, the researchers suggest a ‘sweet spot’ is a ratio of 0.8-1.3 and over 1.5 is a ‘danger zone’ as seen below.
Now to be fair this is a VERY inexact science (and likely why the suggested ratio is so wide). However, as far as I know, it is the first reasonably useful systematic approach to help a coach guide an athlete’s workload. And for rehabber’s it is an EXTREMELY useful tool to guide introduction and progression of load related to injury recovery.
If you stuck with me and made it this long, first off congratulations. Second, you likely have a number of questions….I know I did when was reading this literature. I even went as far as emailing the two primary authors, who are amazing and replied to me from the other side of the world within 24 hours. How accurate is the golden rule of 10% increases in running volume weekly? Is there science to back this? What about pre-season versus in-season versus late season workload? What about a fatigued athlete? All great ideas for future blogs.