Thoracic (mid-back) Mobility
Our modern day workplaces and lifestyles have increasingly involved seated and sedentary versus upright posture. This postural evolution (or more appropriately de-evolution) makes normal thoracic function and mobility an uphill climb for many of us. Limited thoracic spine mobility has a broad spectrum of implications from efficient energy transfer for professional athlete’s to difficulty breathing later in life.
Recent research has noted the connection between the thoracic spine (mid back) and shoulder pain/impingement, neck pain and adhesive capsulitis to name a few. The theory is regional interdependence, fancy medical terminology for what astute clinicians have known for years: dysfunction in one area of the body results in predictable compensations in nearby joints and tissue.
Three examples of the potential consequences of thoracic mobility limitations are briefly discussed below.
An office worker spends the majority of their day at a computer and minimal relief time from the office chair. Long work days often make it difficult for these individuals to fit exercise into their schedule. Eventually a progressively stressful posture combined with inactivity may contribute to a rigid mid back and neck pain due to excessive strain on the cervical musculature.
The manual laborer frequently works overhead or in tight quarters. The loading/demands on the shoulder are often so extreme that any deficiency in shoulder functioning can have catastrophic consequences. Poor thoracic mobility may prevent optimal orientation of the shoulder blade (scapula) resulting in ongoing/recurrent shoulder impingement and an eventual rotator cuff tear.
loading/demands on the shoulder are often so extreme that any deficiency in shoulder functioning can have catastrophic consequences. Poor thoracic mobility may prevent optimal orientation of the shoulder blade (scapula) resulting in ongoing/recurrent shoulder impingement and an eventual rotator cuff tear.
In the pitcher, or other overhead athlete, poor thoracic rotation will necessitate greater  mobility requirements from the already taxed shoulder and elbow. An overhead athlete will only be able to compensate for so long to maintain performance (ie. pitching velocity) before their shoulder and/or elbow and/or wrist breaks down. Just mentioning the words labral tear or Tommy John surgery around a pitcher makes them want to do their thoracic mobility work as part of their arm care.on the shoulder are often so extreme that any deficiency in shoulder functioning can have catastrophic consequences. Poor thoracic mobility may prevent optimal orientation of the shoulder blade (scapula) resulting in ongoing/recurrent shoulder impingement and an eventual rotator cuff tear.
mobility requirements from the already taxed shoulder and elbow. An overhead athlete will only be able to compensate for so long to maintain performance (ie. pitching velocity) before their shoulder and/or elbow and/or wrist breaks down. Just mentioning the words labral tear or Tommy John surgery around a pitcher makes them want to do their thoracic mobility work as part of their arm care.on the shoulder are often so extreme that any deficiency in shoulder functioning can have catastrophic consequences. Poor thoracic mobility may prevent optimal orientation of the shoulder blade (scapula) resulting in ongoing/recurrent shoulder impingement and an eventual rotator cuff tear.
For those of us that work in the manual therapy/Sports Medicine/musculoskeletal world, cases like these are an almost daily occurrence. The thoracic spine is a common area requiring passive (manual therapy, mobilization/manipulation) and active (therapeutic exercise) intervention even if it is not the primary point of pain or concern.
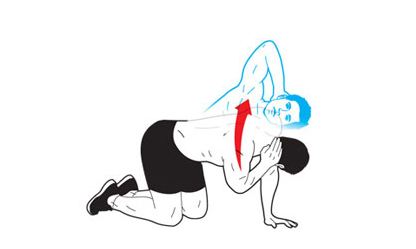
Give the following thoracic mobility exercises a try! Thoracic Mobility: Extension Thoracic Mobility: Rotation
(Note: there are infinite number of thoracic mobility exercises/variations available on the web, you tube etc…these are just a couple options to get you started!).